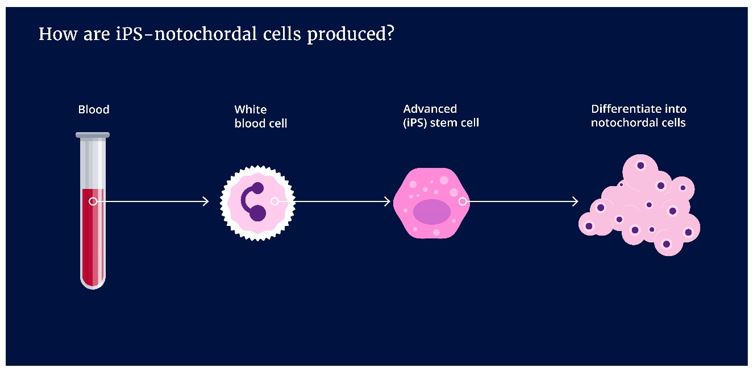
Yes, the advanced stem cells being developed are derived from human. The advanced stem cells in this project are called induced pluripotent stem cells. This is abbreviated as iPS cells. iPS cells are generated in the laboratory.
White blood cells are programmed in the laboratory to revert from a fully developed state back to embryonic stem cells. iPS cells can multiply themselves well, making them ideal to make enough cells for the large population of patients suffering from degenerative discopathy. The iPS cells are re-programmed to notochordal cells, the potent cells only present in young and healthy discs.
It is not forbidden by law. We do not use human notochordal cells because these would need to be collected from human embryos and children. Next to the ethical concerns, such sources are not broadly available for the millions of patients that need treatement against back pain. Furthermore, to date, the available technology does not support amplification of human notochordal cells in the laboratory. The notochordal cells loose their identity when being amplified.
In patient care, preventive treatments are only considered as a possibility once they have proven efficacy to work. The iPSpine approach that is being developed is intended for therapeutic purposes. The project encompasses laboratory and preclinical work to further develop the envisioned advanced therapy. The project focuses on addressing biology questions that help us understand the mode of action of the advanced stem cells and their interaction with the biomaterials and the disc tissue where they will be implanted. The foremost activities are centered on safety and possible efficacy of the engineered cells in combination with the smart biomaterials.
There are additional aspects that would need to be addressed to consider the developed strategy for preventive therapy in patients that may be at risk to develop disc degeneration. The concerns about safety there are even more stringent and carry ethical challenges.
A difficulty with understanding whether a treatment could be used preventively is that it needs to be tested for multiple years in order to get insights in uncertain and unknown side-effects and whether it is effective as a preventive treatment. Only once a wide population of patients has been treated may these scarce and expected side effects be observed. The difficulty lies in how severe a person’s lower back pain will become if he or she will not be treated and what the long-term differences are between having a preventive iPSpine treatment, an alternative treatment and no treatment. Such research will as well bring insights in whether iPSpine as a preventive treatment is proportional in terms of efficacy and side-effects for the (future) pain it is trying to relieve or alleviate. Another consideration would be what the alternatives are. When there are alternatives with fewer side-effects, that are less invasive and/or financially less costly, it could be possible that these alternatives will be preferred. The availability of iPSpine as a preventive treatment will as well depend on whether health insurances will cover the costs of a preventive treatment when other healthcare costs might be more urgent. Altogether, these considerations imply that the iPSpine treatment needs initially be considered as a therapeutic application once clinical signs are at play.
NC Biomatrix is a company that is commercializing the use of a molecular treatment product for disc degeneration that is based on the tissue found in the center of pig discs. iPSpine is exploring the use of a similar base material in combination with other biomaterials and with advanced stem cells which in essence are notochordal cells engineered in the laboratory with technology that the iPSpine project develops. iPSpine hopes that the base material will help to recapitulate the healthy environment and provide the engineered cells with safe cues which flourish within the disc. Also by combining it with other biomaterials we hope to enhance its biomechanics restoring properties. The product of NC Biomatrix is a simpler approach which can be translated more quickly but will only address individuals with early to moderate disc degeneration. It may also be used prophylactically. The iPSpine product is more complex and will take much longer to reach the clinic but is inherently more powerful and will address a much larger population of patients with even severe disease because of its use of cells.
If a disc is herniated, there is a chance of the hydrogel to leak out. Technically the immune system will be exposed to a foreign body material, i.e., the “foreign” iPS juvenile disc cells, and a local immune reaction may occur. Therefore, the treatment is not suitable for patients suffering from an acute herniated disc.
The iPSpine project starts with the understanding that as long the disc is intact the disc environment remains protected from the immune system. The degenerate disc is considered intact if the content from the center of the disc has not herniated through the outer layer. As such, it is expected that the immune system will not get in touch with the “foreign” iPS juvenile disc cells. While iPSpine will study these iPS juvenile disc cells in clinically relevant animal models, parallel research activities focus on whether it is possible to bypass a possible immune response. The first steps are undertaken in the laboratory to also study modified iPS cells that have been engineered to not elicit an allergic response even if they would come in contact with the immune system.
In all vertebrates there is structure resembling a flexible stock that extends throughout the body of the embryo. This structure is called the notochord. The notochord ensures firmness and gives signals that drive the development of the embryo. It is temporary; the notochord disappears and at some point, when the development of the spine is complete, notochordal cells only reside is in the center of the disc.
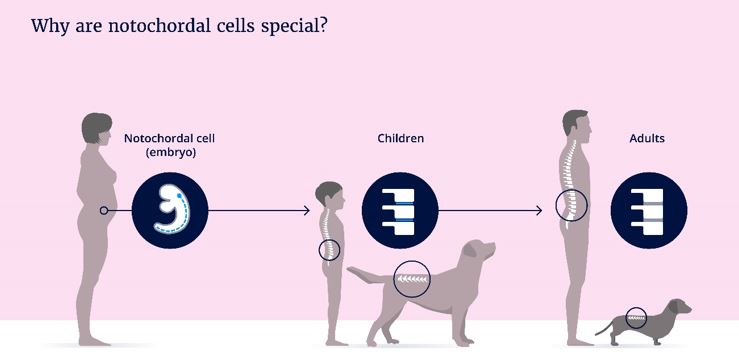
There is something very special about notochordal cells.
Notochordal cells are present in children but disappear later in life. It happens, to what extent it is a coincidence, that 80% of people suffer from back pain once in their lives . Similar problems occur also in our 4-legged family-members; the dog. The problem mostly occurs in dog breeds with relatively short legs, such as the Dachshund, that often suffers from a acute hernia early in life. In other dog breeds, such as the Labrador, the notochordal cells remain present in adult animals and we only see back problems later in life.